After 6 reported deaths and over 400 reported incidents related to oxygen cylinder use the NHS released this patient safety alert (click on image for more details):
These are only the reported cases – the number of true cases will be several magnitudes greater.
Father of two, Roland Bull, died in his sons arms within 15 minutes of discharge from hospital – the oxygen cylinder he was attached to while appearing to be delivering oxygen actually wasn’t (see here).
The healthcare front line is a highly complex environment with a constantly renewing and fluctuating workforce. Designs which don’t pay respect to this can be deadly. Further, within this complexity, alerts and training can be extremely weak interventions for improving safety.
‘We cannot mitigate slips and lapses through better training. Errors will be repeated unless the system is redesigned’.
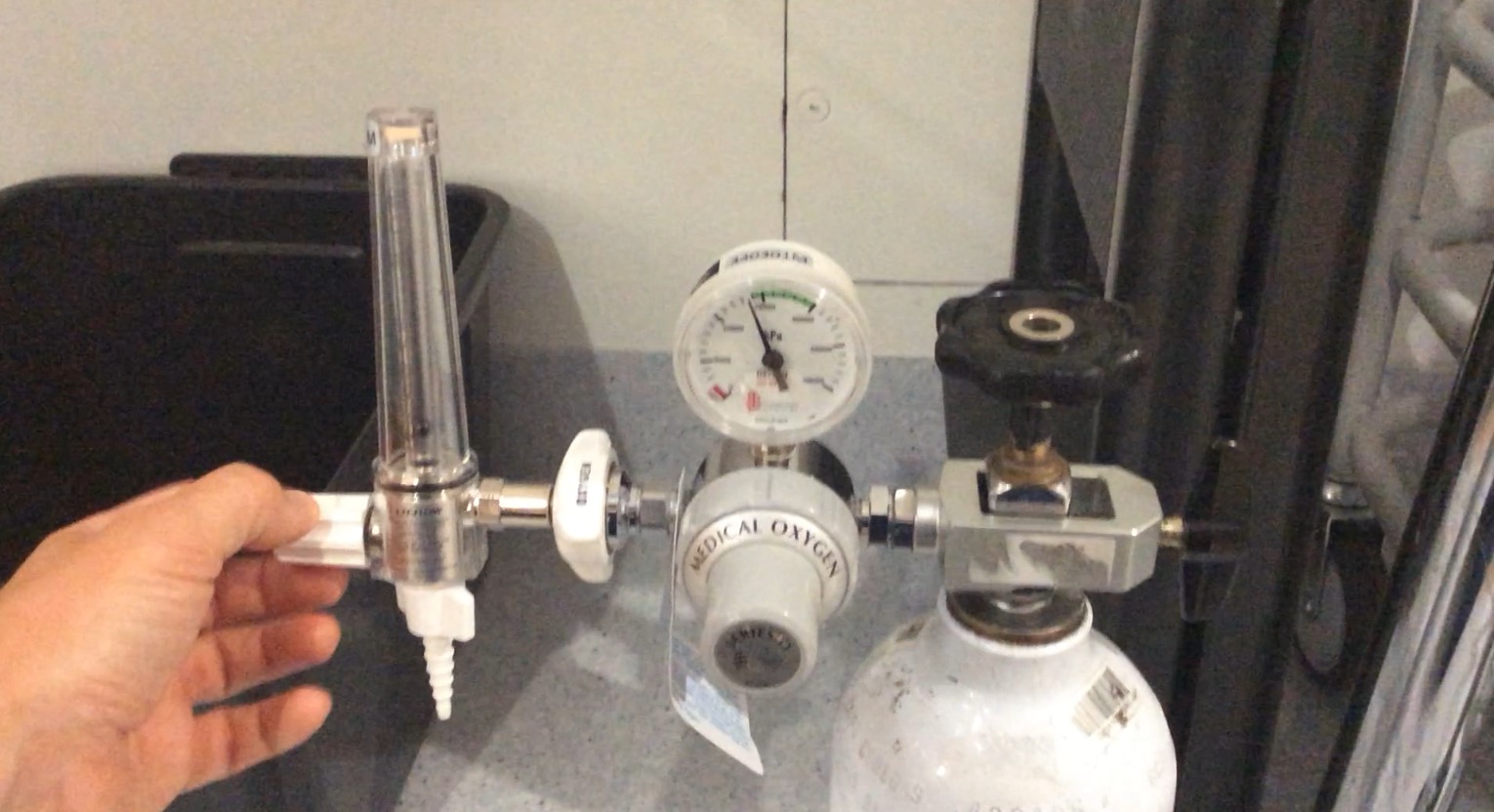
There are numerous design features inherent to the oxygen cylinders which impair their appropriate operation
1. A fairly non-descript grey cover over the dial for turning the cylinder open or closed in effect hiding it – one may assume there is nothing underneath.


2. When the open/close dial is turned to open there is no feedback to indicate this has actually been performed. Any feedback from the cylinder itself may tend to suggest to the user that is open irrespective of whether it is in the open/closed position.
3. The cylinder gauge indicating how much oxygen is in the tank – in the green zone – a user may believe this indicates the cylinder is open.

4. The flow dial on the top of the cylinder can be dialled to deliver flow irrespective of whether gas flow is being delivered (more feedback suggestive that the cylinder is open irrespective of whether the cylinder is actually open or closed)

5. Even when the cylinder is turned to closed when the flow dial is turned up to deliver flow an audible hiss of gas may be heard for a second or so suggesting the cylinder is open.
6. Instruction on the collar of the oxygen cylinder itself are in extremely small font, placed away from their location of importance and readily obscured by straps used to retain cylinders.


Within complex health care work environments these design peculiarities lead staff to fail to operate the cylinders appropriately.
Until the cylinders are redesigned patients and front line staff will continue to suffer unnecessarily.
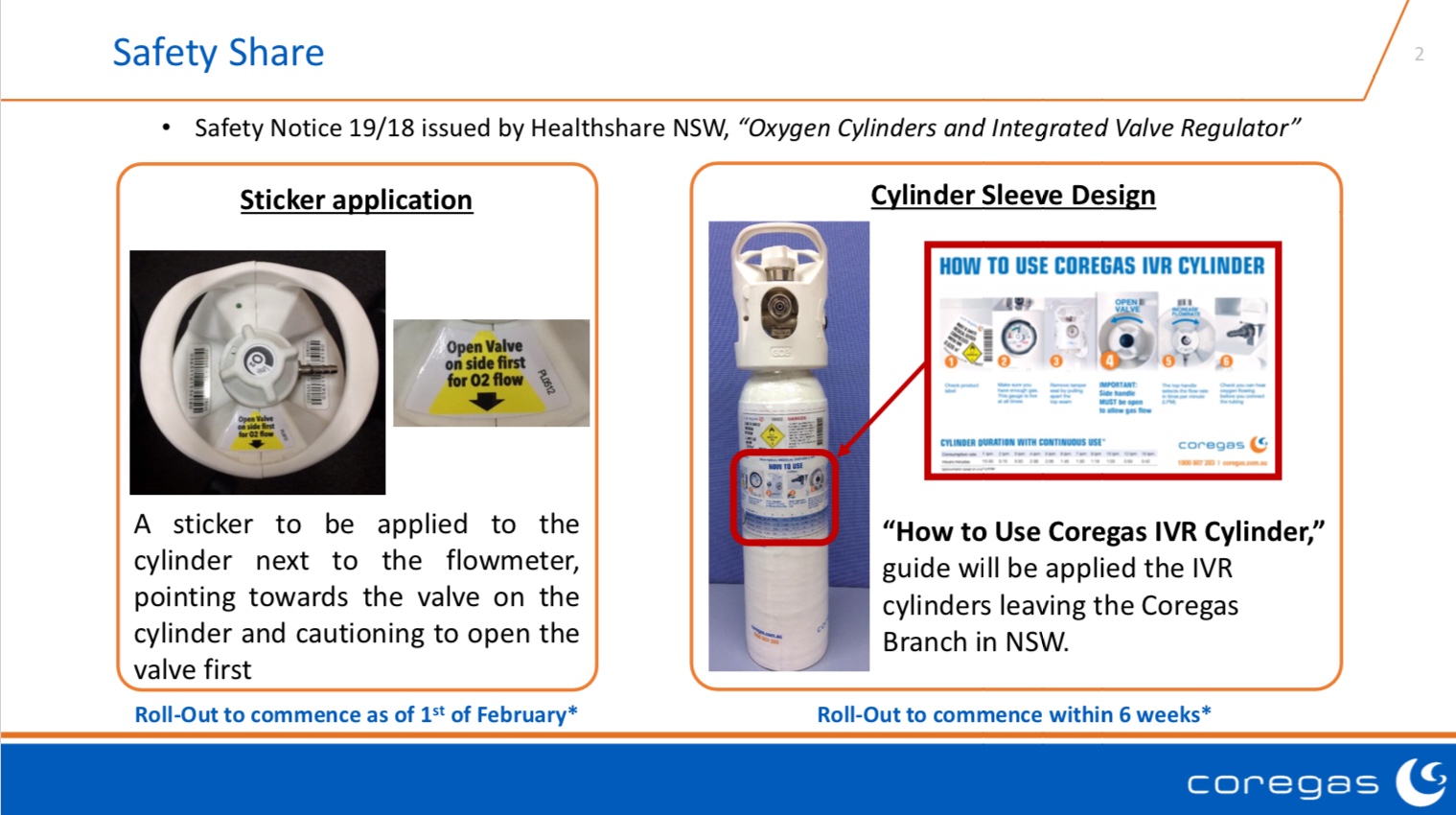
Temporary measures could include labelling over the open/close valve cover instructing it be removed & the dial turned to open before cylinder use. Similar labelling is used in industries with good understanding of human factors and system safety.

Future designs could integrate the the two dials into one, ensuring the cylinder could be turned to open easily and only appear to be providing oxygen flow when it actually is delivering oxygen flow.
The images above show BOC cylinders. Air Liquide supply another style of oxygen cylinder which overcomes many of the issue related to the BOC cylinder (have integrated two dials into one & unable to turn flow dial to deliver flow without cylinder being open). However the Air Liquide cylinder also has its own severe design issue – it delivers no flow if the flow dial is set between two numbers – please watch video below.

We have yet to hear anything from cylinder manufacturers regarding redesign. We will be sure to keep you updated.
This is a video demonstrating the functionality of some of the older oxygen cylinders still in use. While they may not look as pretty their design makes them intuitive – it is readily obvious if oxygen is flowing or not:

Should we be removing the newer integrated valve design cylinders from the front line unless they come with a reliable flow indicator?
If patient safety is to improve we need a much greater understanding of human factors and system safety in healthcare.
Much of the equipment we interface with on the front line may appear to be okay until humans interact with it. However, when we reveal how dangerous poorly designed equipment is, our systems for removing or improving it are severely lacking.
As complexity on the front line increases unchecked so too does our adverse event rate:

Front line staff need to be empowered to improve their work environments – when this happens patient safety will improve.
We are still to hear from BOC or Air Liquide regarding improvements to their cylinders. In the meantime the best we can do is ask that you forward this post to your hospital procurement staff and ask that they consider purchasing either the older cylinders or cylinders from manufacturers who consider human factors in their design:
This Linde Integrated Valve LiV IQ appears to have overcome many of the human factors issues discussed above. Looking forward to trialling one.

Towards the beginning of 2019 an alert and point of care label notifying staff of this issue was added to CoreGas oxygen cylinders:
11 Comments