Preox ETO2 trial (?POETO trial)
Perhaps a useful way to trial the ETO2 would be to blind the proceduralist to the number,initially. Obviously they would know they are being assessed and this might impact on their performance. The proceduralist could preoxygenate the patient as they normally would and would call out when they felt the patient was sufficiently preoxygenated and are ready to induce the patient.
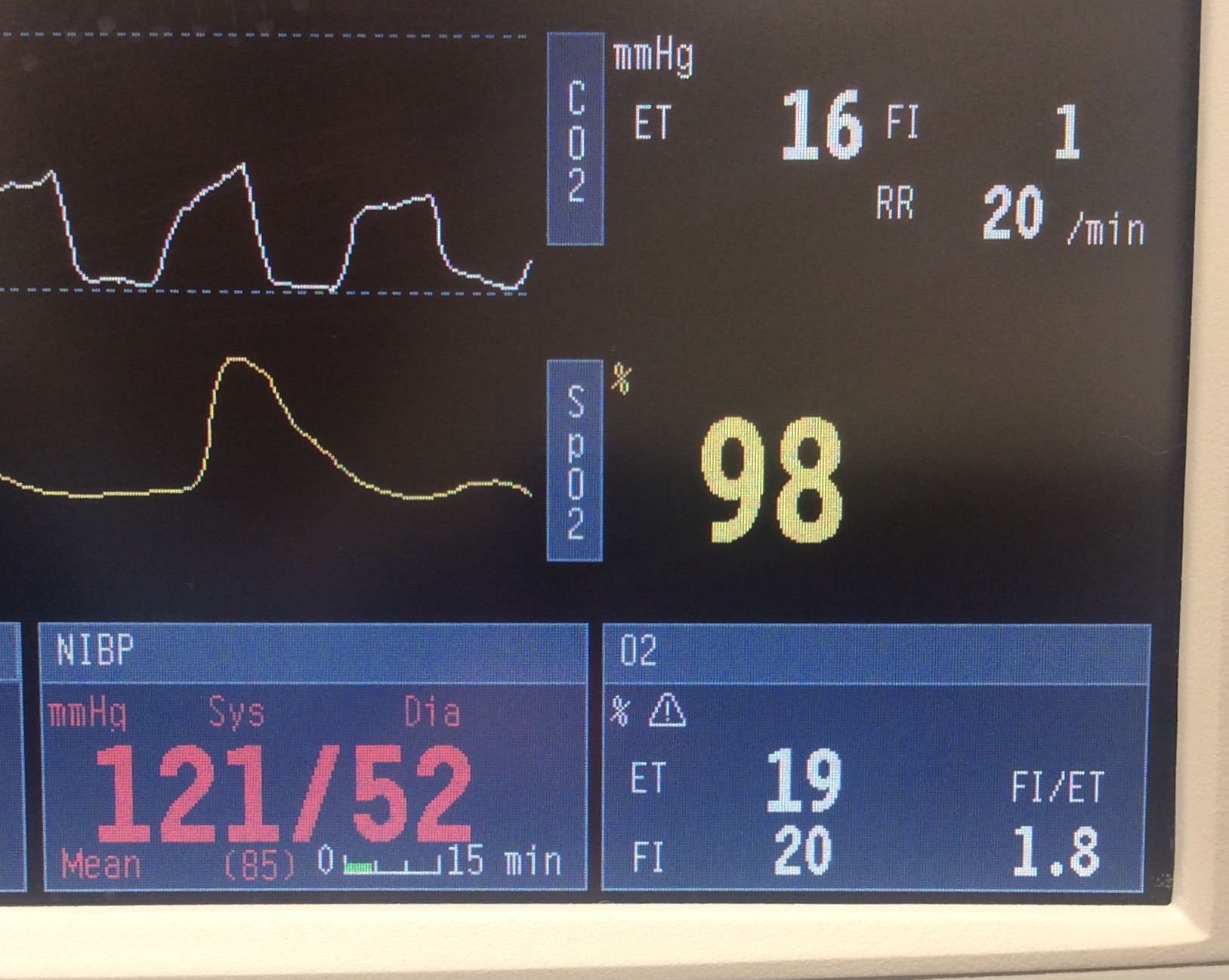
The observer could then let them know what the ETO2 was – if its high enough (80 to 90s) go ahead and induce.
If not high enough the time could be measured until it reaches the appropriate ETO2 for induction. Comments could also be provided for each case as to why it was felt sufficient ETO2 not reached. We could create a list of potential reasons:
– Pipeline mix ups
– Forgetting to connect to oxygen source
– Connecting to air instead of oxygen
– Inadequate O2 flow rate e.g. unrecognised empty oxygen cylinder
– Use of BVM without expiratory valve
– Poor technique of choice
– Unintended mask leak (e.g. using NC or PEEP valves)
– Unrecognized airway obstruction
– Unrecognized impaired minute ventilation
– Insufficient length of time for pre-oxygenation
– Other (please provide comment)
If obvious reason for poor pre-oxygenation noted by observer, this could be relayed at any stage to the proceduralist, time recorded from commencement of preox at which proceduralist informed and reason recorded.
Could be performed for all RSI (and any anaesthetic GA induction)
Indication for RSI noted (it would be helpful to generate a list of these)
Method of pre-oxygenation recorded (Mapleson C, BVM does it have exp valve +/- PEEP valve, anaesthetic machine circle circuit / T piece Circuit, NIV, THRIVE, NRM+/-NP with ability to record flow rates administered e.g. flush rate, 15L/min)
NP applied at any stage (Y/N)
Is positive pressure mask ventilation administered in the period between induction and intubation.
Minimum O2 sats attained during period from commencement of preox until successful intubation along with time at which this occurred after commencing preox (it may be lowest at the start of preoxygenation)
This is something that we might easily be able to set up and could run as a multicentre trial in ED, ICU, and anaesthetics.
Would potentially look at creating an app which allows data be rapidly entered from centres throughout the world and we could all observe the results as they come in in real time. Perhaps this could be funded by the companies making ETO2 compatible monitors – given there appears to be at least 3 of them (Masimo, Philips, GE) this may not be viewed as collusion? We could also get them to supply the equipment for trial for free.
Very interested in your thoughts