Point 1 – The significant issue of Central Line Related Air Emboli persists despite measures already adopted – all cases are iatrogenic and avoidable
The issue of iatrogenic central line related air emboli persists despite measures which have been put in place. The magnitude of this issue is not to be underestimated – a recent meeting of the Intensive Care Network agreed that worldwide around 1 person dies every day from this avoidable issue. The evidence to back this statement can be reviewed here.
As can be seen 1 a day may be a substantial underestimate – it may be in the region of 7 deaths every day in the US alone. Regardless of the true figure all cases are avoidable.
Many cases occur as a result of accidental line mis-connection (there have been several cases like this at St Elsewhere). This is a worldwide phenomenon – the solution posed here by RCOA is relatively ineffective given the complexity of our work environments.
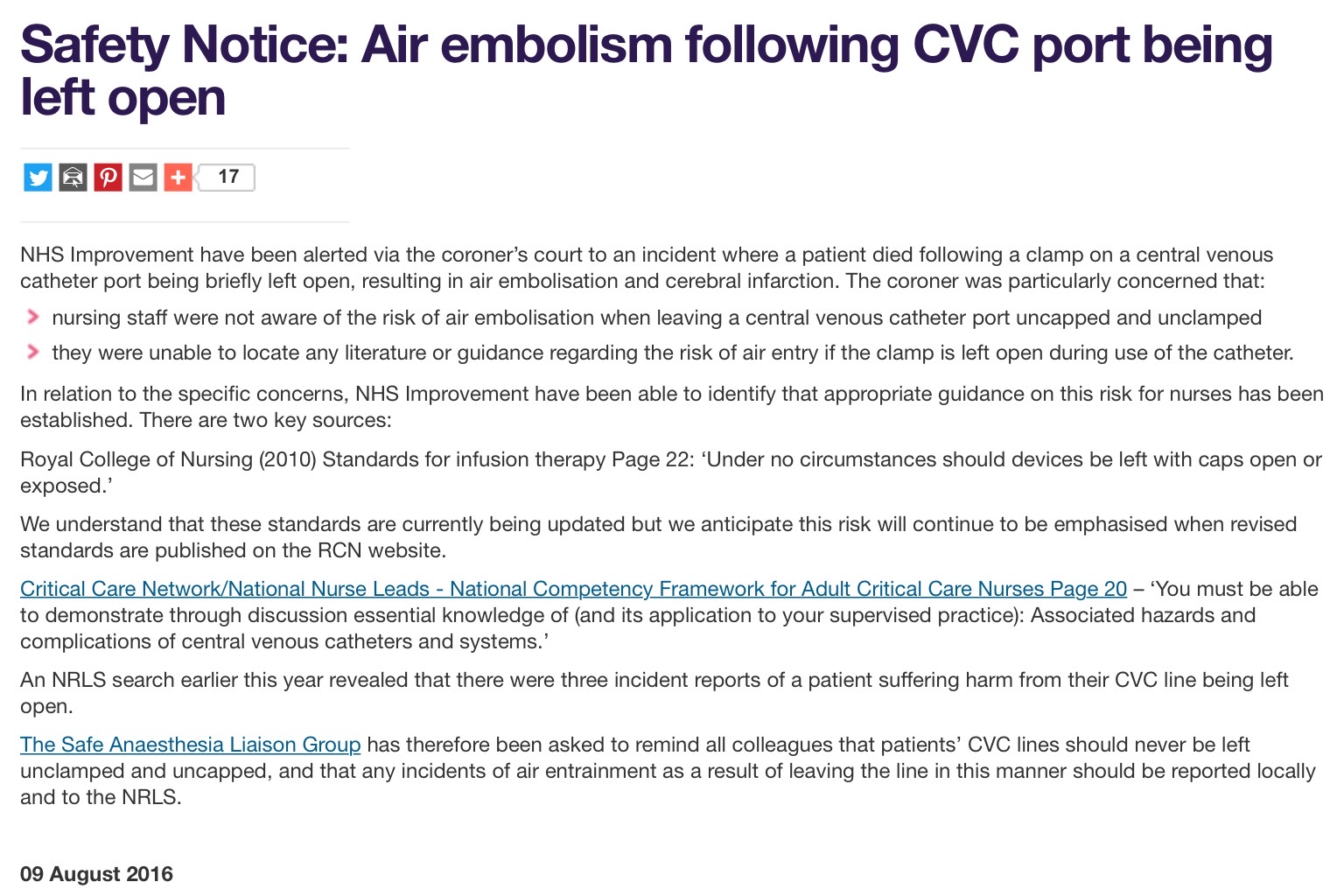
There is potential to engineer out these cases of air embolism from accidental misconnection using a highly effective forcing function i.e. preventing staff from accidentally leaving central lines open to air.
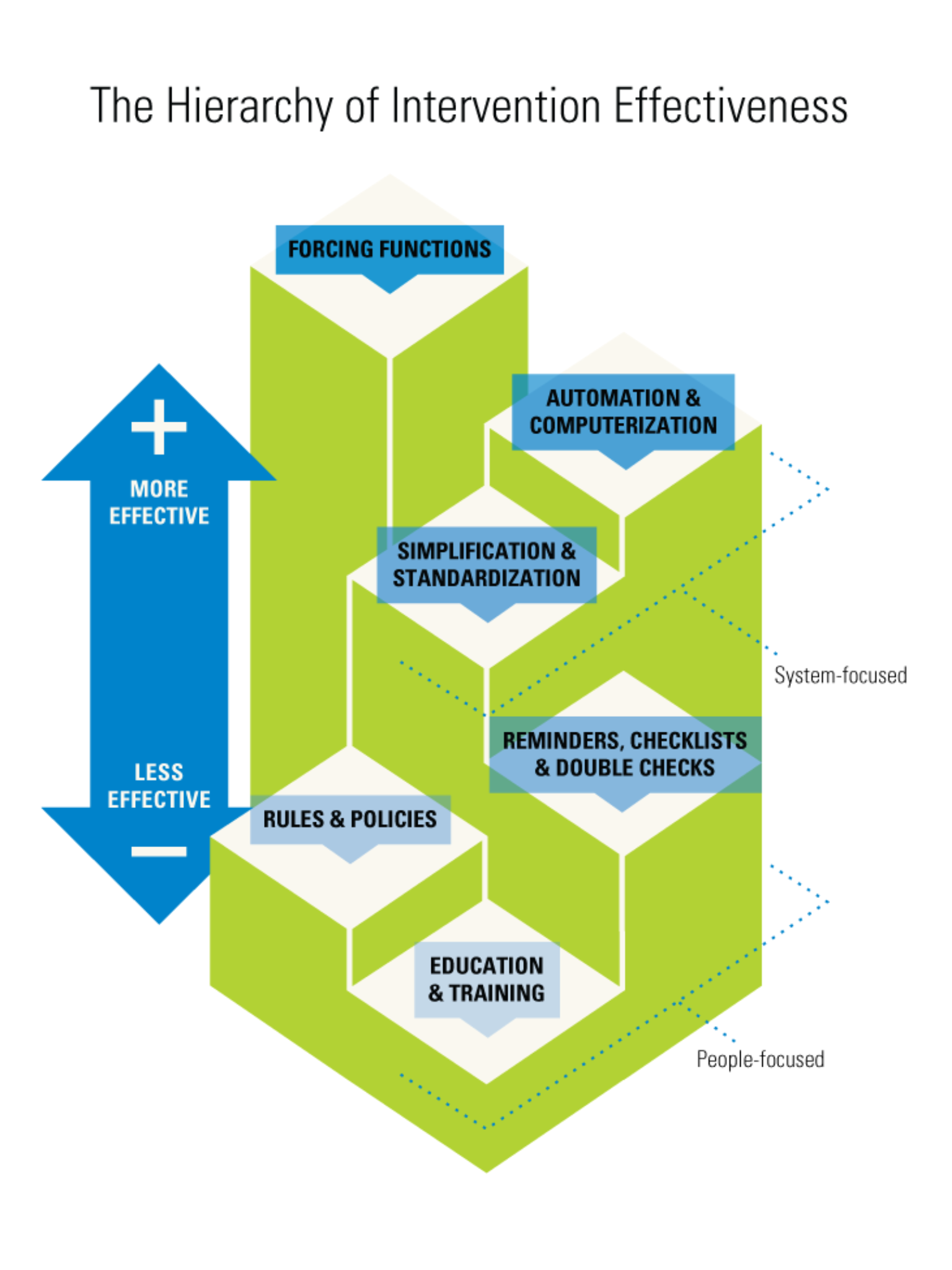
Point 2 – CEC NSW sent out a request to industry for lines and attachments with bonded valves in August 2015
In August 2015 based on this human factors understanding the NSW CEC sent out a request to industry looking for central lines and attachments with bonded valves to address this issue. See below:
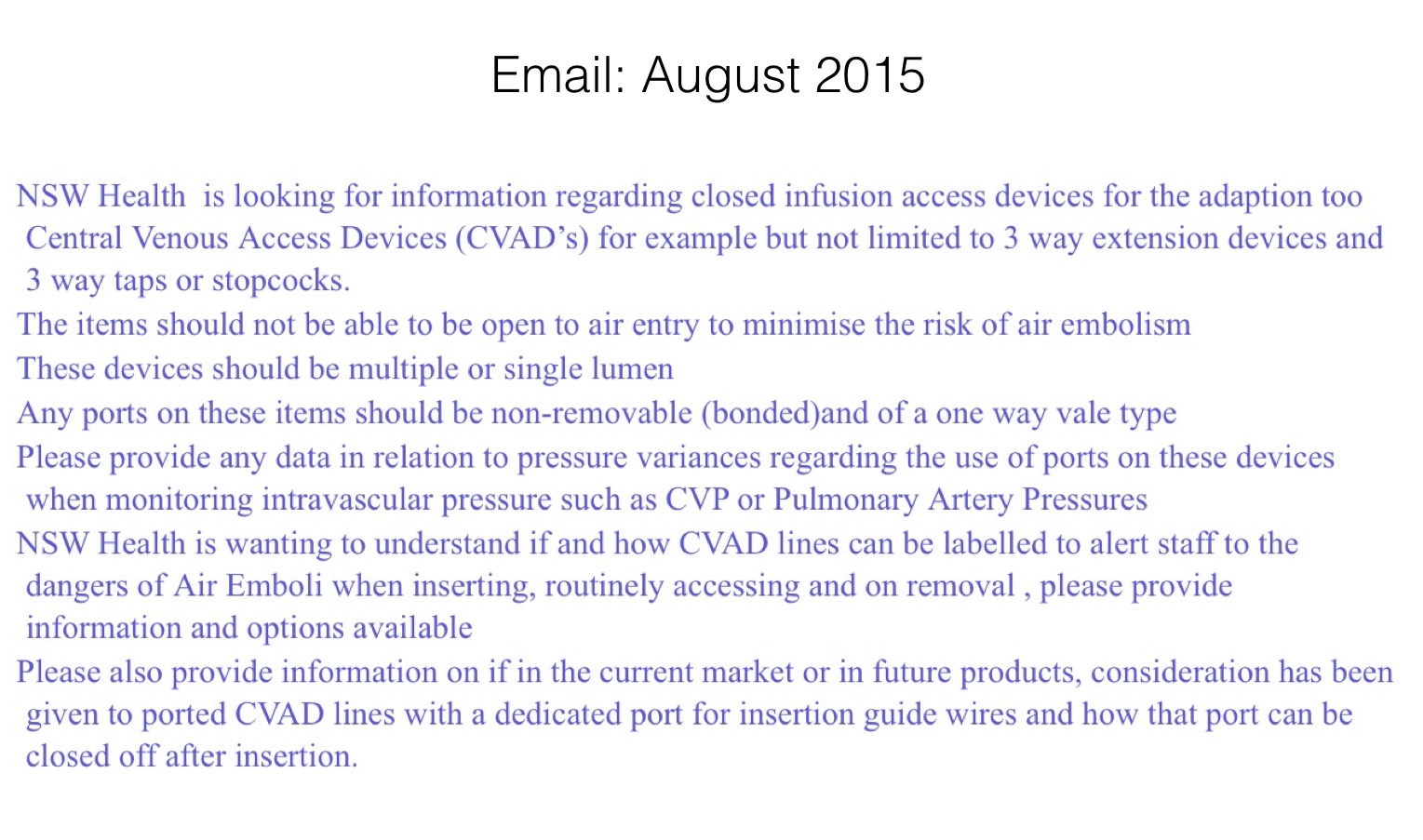
Point 3 – The Kimal Altius central line has these properties
The Kimal Altius CVC received TGA approval in October 2016
To our knowledge as yet this line has no been trialled in Australia though hospitals aware of the significant of central line air emboli (including Nepean) are looking to trial the Kimal Altius line.
Point 4 – Important not to replace one issue with another
The Kimal Altius has been and is used in many institutions throughout the world. It was introduced in 2014 and so far 92,000 units have been sold: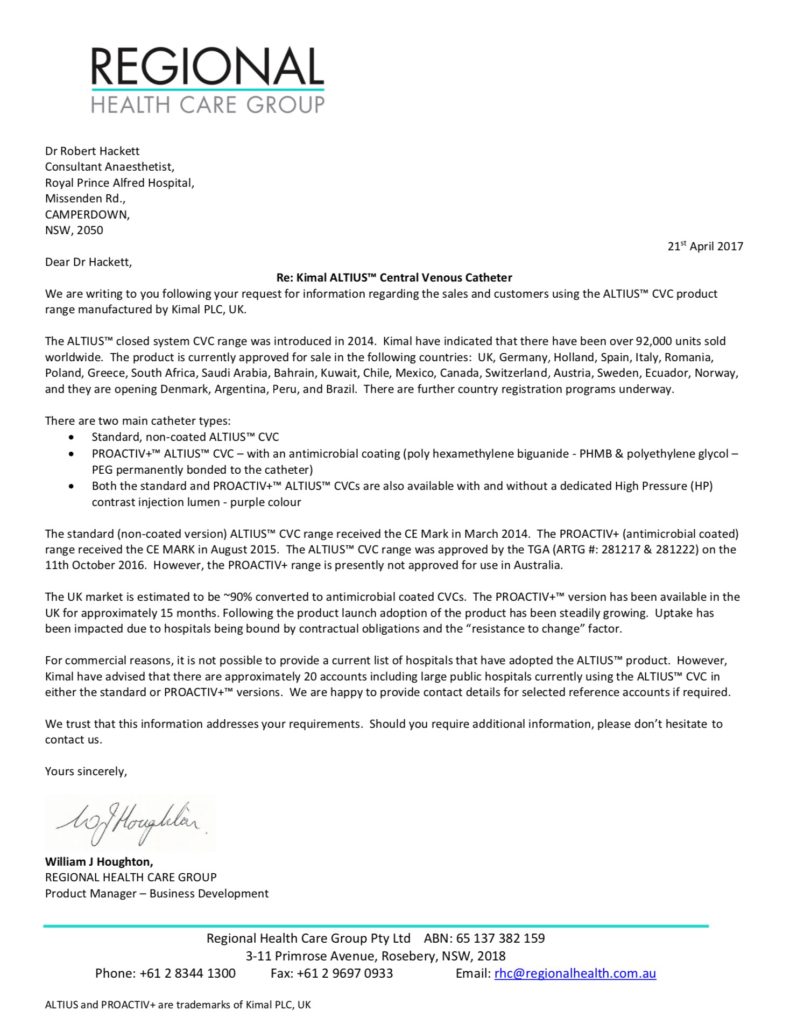
We have received positive feedback from several institutions already using the line (see here)
Several critical care staff have offered to be contacted directly to provide feedback about these lines:
From Duncan.Wyncoll@gstt.nhs.uk :
We have been using these lines for about 8 months (used about 500+) and so far I think we are generally fairly happy. However, we would still regard ourselves in an evaluation phase!
This is our take on them:
1. To be brutally honest we mainly changed to them because we wanted a 5-lumen line and the Altius/Kimal was the cheapest of the ones we were looking at – Vygon and Cook were between £8-40 more per line.
2. The antimicrobial aspect is important to us since our CRBSI rate is low at <0.5/1000 catheter days, and we did not want to see an adverse trend. We do not know yet whether they are better or worse than our previous Vygon Expert Quad, and this will take a while to be statistically sure.
3. The doctors really like the nitinol wire as standard and also like the device which feeds the wire through the catheter.
4. The high pressure purple line is a major advantage to us since we do CT scans frequently etc
5. The nurses DO NOT like the fact that they cannot see through the lines and this has caused some concerns with them. Not sure it is a major issue, but they did take a lot of persuading to continue!
6. The integrated bungs saves more money but again it was an issue with the nurses because they sometimes struggle to appreciate changes like this. They also were unsure in not having a line clamp.
7. The only occasional problem we have had with the bungs is that if the male insertion part is not fully inserted then the valve may not be fully open and injecting can be harder…
As I said earlier we are well up the learning curve but still have a little way to go.
Hope this helps,
Dr Nhi Nguyen Intensivist at Nepean is aware of the value of closed system CVCs – they would like to trial the Kimal CVC:
Awaiting Testimony from: michael.stoller@web.de
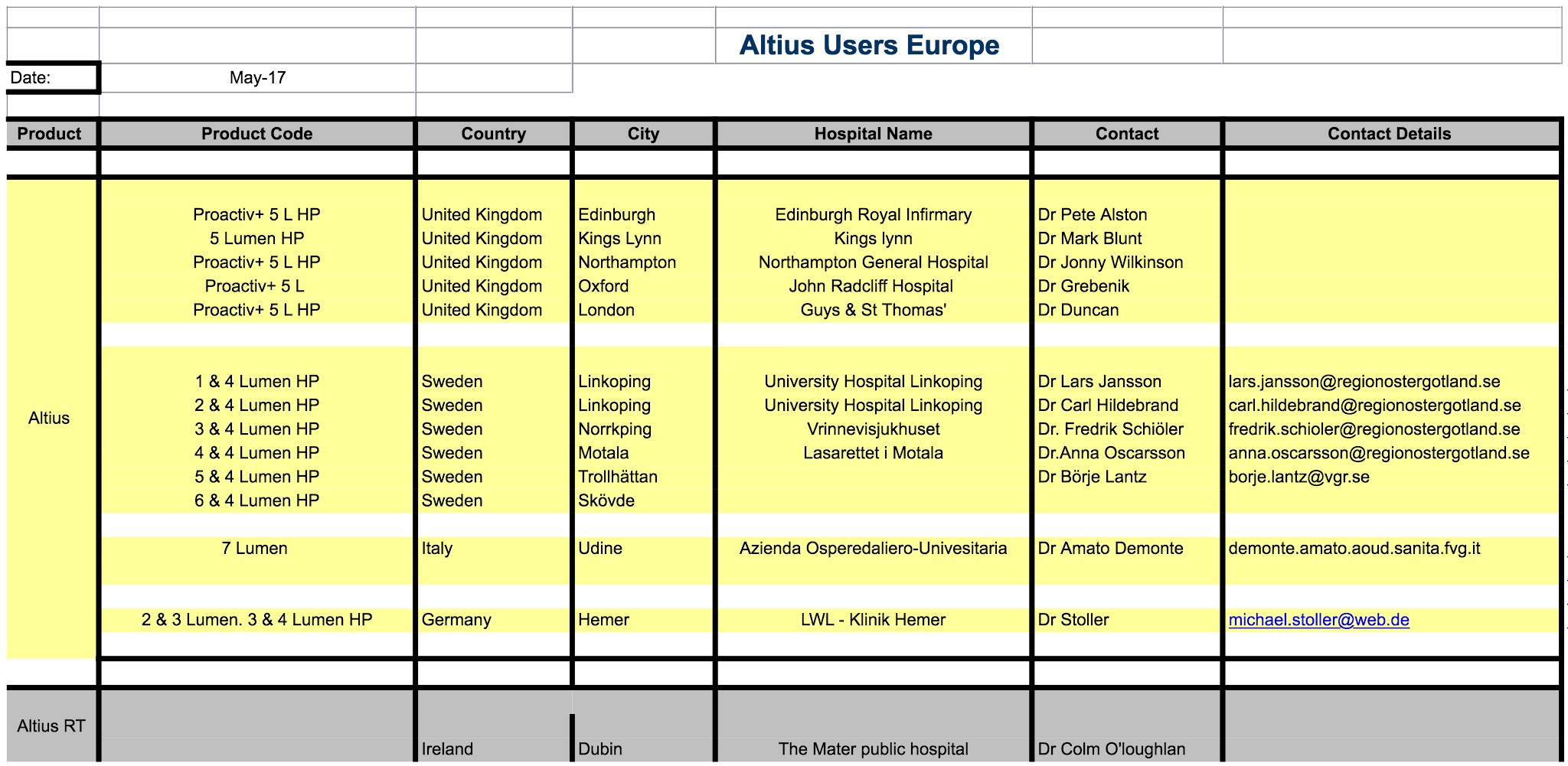
Further users in Europe willing to provide feedback:
Obvious differences with the Kimal central line include
1. An opaque proximal portion to the line – we have asked for direct feedback from nursing staff who have been using th eline elsewhere in the world to see if they feel this is still a concern.
2. Lack of proximal clamp – the presence of bonded valves means that a proximal clamp is not required for each lumen. Proximal clamps have caused issue – there was a recent case of central line rupture because a clamp was closed when a high pressure contrast injection was administered to the line.
3. The round lumens of the central lines offer less resistance and higher flow rates for the same gauge of catheter compared to the Arrow lines we currently use.
4. Bonded valves. This is a property the CEC sent out a request to industry to find. The CEC also wrote policy guidelines regarding central line management – an interpretation of these guidelines has been given as reason from the infectious disease department to not support use of the Kimal Altius lines – I have discussed this issue directly with Xthe authorX (both the main author of the policy documents and the request to industry regarding central lines with bonded valves) – it is her opinion that as the valves are bonded to the lines they do not constitute a removable attachment (such as a giving set) which the policy guidelines suggest should be removed every 4 to 7 days.
Point 5 – Infection Rates
Current evidence supports the use of simple split septum valves (as seen on Kimal Altius line) in reducing CLABSI over the current more complex valves that are often applied to central lines at St Elsewhere (see here)

Evidence indicates that frequent change of removable valve attachment sites may increase CLABSI (see here).
Evidence also indicates that traditional open lumens for valve attachment are more difficult to decontaminate (see here).
One reason given for preventing a trial of central lines with bonded valves is that there are policy guidelines (from CEC NSW – the same people who sent out a request to industry for central lines with bonded valves) indicating that any attachments to the central line need to be replaced every 4 to 7 days. However the bonded valves are not an attachment they are bonded on and also CDC guidelines from 2002 indicate that short extensions on the central lines do not have to be replaced:
Point 6 – Cost
The suppliers of Kimal Altius have offered to supply 40 high pressure injectable CVCs for trial.
Use of Kimal Altius Central Lines will deliver a front end cost saving – the cost of the lines is equivalent to those we are currently using and we will not need to expend additional money on additional valves for attachment.
Use of Kimal Altius Central Lines have potential to offer vast back end cost savings – sums of up to $US30 million have been payed out for individual cases of central line related air emboli.
Point 7 – Staff familiarity, education, issues raised – opaque proximal end, lack of clamp.
The suppliers of Kimal Altius have offered to provide their full and ongoing support to ensure that staff have 24/7 lines of communication, and staff are completely educated and orientated with using the lines prior to any trial.