Recently a tragic mix up where oxygen tubing was connected to a urinary catheter resulted in the death of ex-Socceroo Steve Herczeg (see here).
‘How can anyone make this mistake?’
Unfortunately events like this occur regularly – we often only here of them via the media – our error report systems lacking transparency (see here).
This link from the FDA (see here) documents numerous similar mis-connections.
Through understanding why these events occur we may be able to prevent them.
We need to understand the healthcare safety problem is not bad people:
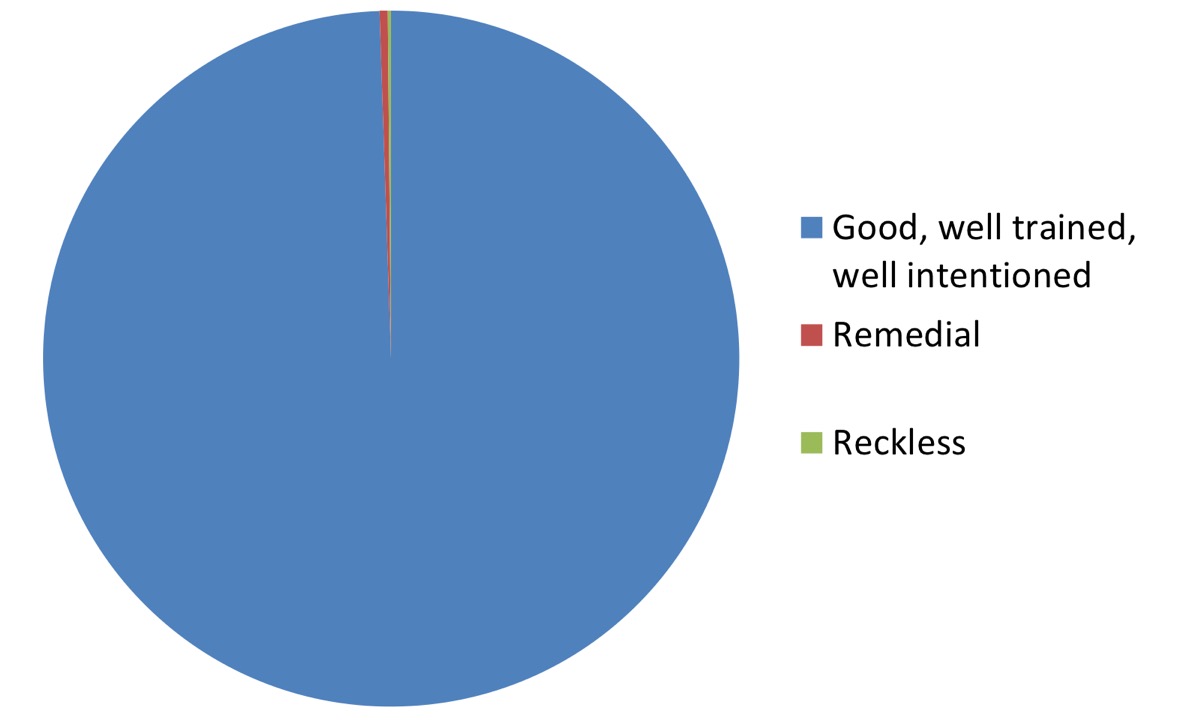
Our hospitals are increasingly complex and humans err. These adverse events will continue to occur if we don’t act wisely.
Line mis-connections can be designed out. The FDA are developing standards for line connections (see here) – similar standards must be adopted worldwide.

Front line staff are often aware of poor system and device design. Given the opportunity and support we can develop simpler, safer work environments, allowing greater focus on patient care. Other industries have adopted six sigma and lean efficiency with great benefit.
Equipment and processes should be assessed through simulated environments, yet still we need the ability to remove hazards even after they’ve reached the front line.
We need the system to be able to learn learn from its mistakes. In Australia this process will frequently involve the Therapeutic and Goods Administration.
The TGA need to be empowered to listen and act on the feedback of front line staff.
For a great introduction to intelligent design please read ‘The Design of Everyday Things’ by Donald Norman
4 Comments